About
Contact
FDA Indications
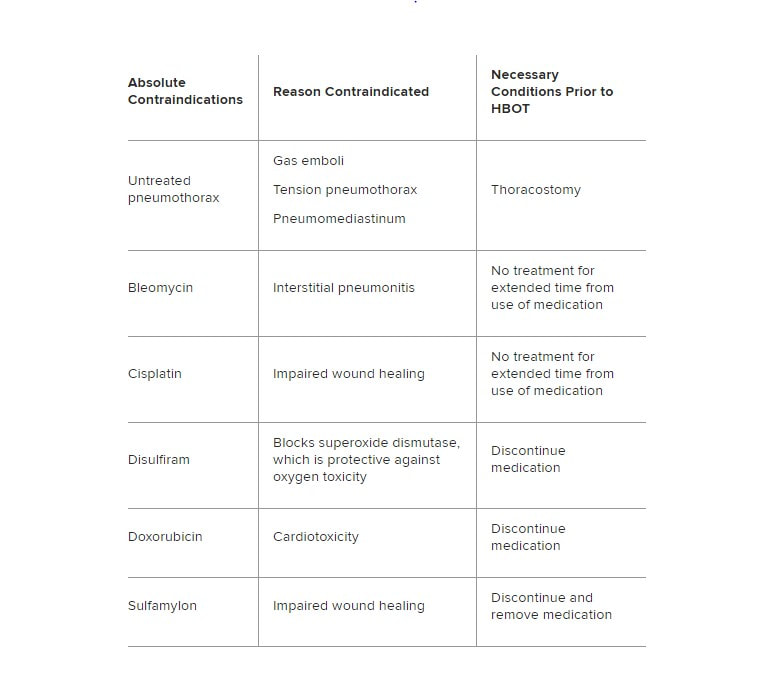
Absolute Contraindications
https://emedicine.medscape.com/article/1464149-overview#a3
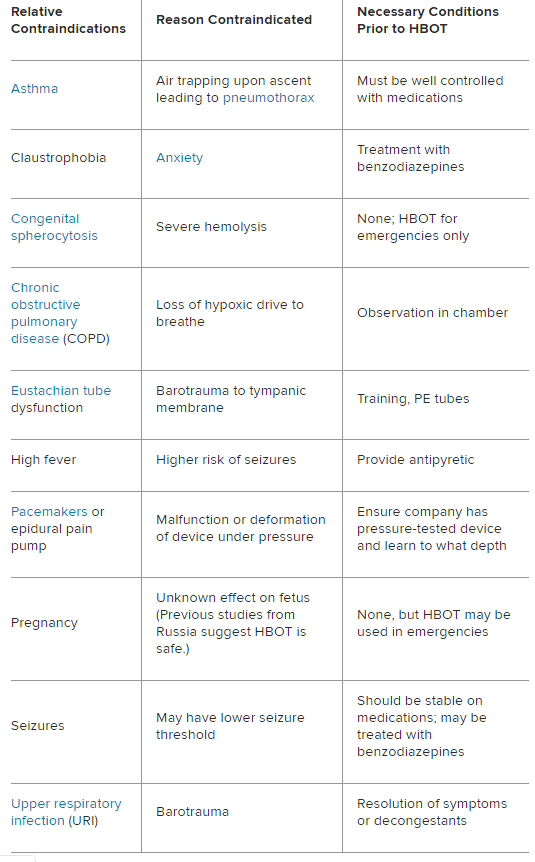
Relative Contraindications
About
Contact
FDA Indications